How to Document Safety Alerts on Your Medication List
When you're managing multiple medications, a simple mistake can lead to serious harm. That's why documenting safety alerts on your medication list isn't just good practice-it's a lifesaving habit. Whether you're a patient keeping track at home or a healthcare worker in a clinic, knowing exactly how to record and act on these alerts makes all the difference.
What Counts as a Safety Alert?
Not every warning on a pill bottle is a safety alert. True safety alerts are tied to high-alert medications-drugs that carry a higher risk of causing serious injury or death if used incorrectly. According to the Institute for Safe Medication Practices (ISMP), these include insulin, opioids, anticoagulants like warfarin, neuromuscular blockers, and oral methotrexate. These aren’t just "strong" drugs; they’re dangerous when dosed wrong. For example, giving methotrexate daily instead of weekly can cause fatal bone marrow suppression. That’s why documentation matters.Each safety alert should include:
- The medication name and strength
- The specific risk (e.g., "Risk of respiratory arrest if given without ventilation")
- The required safeguard (e.g., "Double-check by two licensed staff members")
- How the alert was triggered (e.g., "EHR hard-stop blocked order until oncology indication confirmed")
Just writing "Caution: High Risk" isn’t enough. You need the exact wording from official guidelines. ISMP’s 2024-2025 standards require auxiliary labels on neuromuscular blocker containers to read: "WARNING: CAUSES RESPIRATORY ARREST - PATIENT MUST BE VENTILATED." No shortcuts.
Where and How to Document
Documentation happens in two places: in the patient’s personal record and in the electronic health record (EHR).If you’re a patient, keep a printed or digital list of all your medications. Use a simple template:
- List each drug, dose, and frequency.
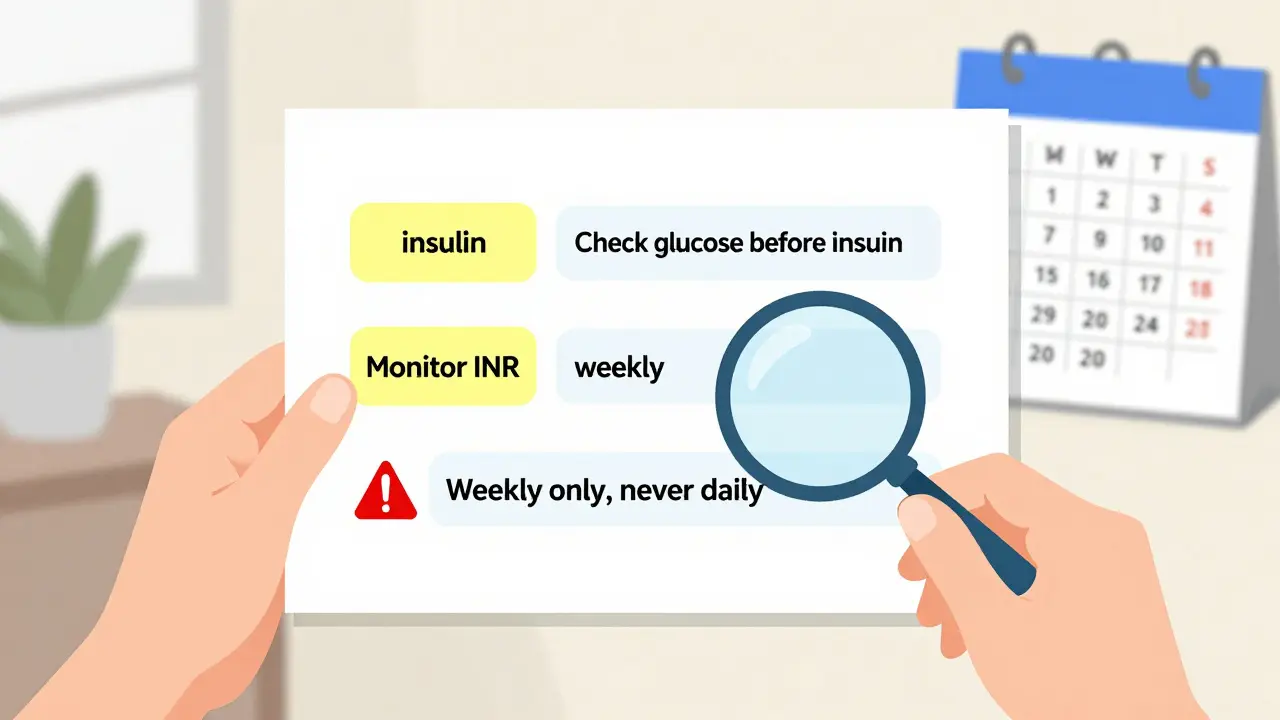
- Next to high-alert drugs, write the safety alert in your own words. Example: "Insulin: Always check blood sugar before dose. Never give if glucose is below 70."
- Include any special instructions: "Must be given with food," "Avoid alcohol," "Requires weekly lab tests."
- Update it every time your provider changes a medication.
In hospitals and clinics, documentation is more structured. EHR systems must be configured with hard-stop alerts-for example, when a prescriber tries to order oral methotrexate daily, the system should block the order and require confirmation of an oncology diagnosis. This isn’t optional. The Joint Commission mandates this as part of its National Patient Safety Goal (NPSG.01.01.01), effective January 2024.
Barcode scanning is another critical layer. When a nurse scans a medication before giving it, the system should cross-check the patient’s list, the drug, the dose, and the timing. If the alert doesn’t match, the system flags it. Facilities that hit 95% scanning compliance see 40% fewer errors. That’s not magic-it’s documentation in action.
Why Ad-Hoc Systems Fail
Many clinics try to save time by just adding a sticky note or relying on EHR pop-ups alone. But research shows this doesn’t work. A 2019 study found that electronic alerts without documented follow-up procedures had a bypass rate of 49%. Nurses and pharmacists get used to clicking "OK" without reading. That’s alert fatigue.The ISMP framework avoids this by layering safeguards:
- Physical labels on containers
- Hard-stop EHR prompts
- Double-check protocols
- Staff training logs
- Monthly safety committee reviews
Each step is documented. Not just "we did it," but "we did it, here’s who did it, when, and what happened." This creates accountability. A 2021 study of 47 hospitals found those with full documentation had medication error rates of 4.2 per 1,000 doses. Those with partial documentation? 12.7 per 1,000.
What to Avoid
Over-documentation is just as dangerous as under-documentation. If every minor side effect triggers a 10-step form, people tune out. Dr. Robert Wachter of UCSF found that systems generating more than 15 alerts per medication order saw compliance drop to 31%. The goal isn’t to record everything-it’s to record what matters.Here’s what to skip:
- Alerts for common side effects like "nausea" or "drowsiness" unless they’re life-threatening in context
- Generic warnings like "Use with caution" without specific actions
- Manual paper logs that aren’t scanned or archived electronically
Instead, focus on alerts that have a clear, actionable response. For insulin: "Confirm patient’s last glucose reading before administration. Document result." That’s it. Clear. Trackable. Actionable.
Real-World Challenges
Even the best systems face hurdles. Rural clinics often lack staff to manage documentation. One pharmacist on Reddit shared: "We’re supposed to document every bypassed alert, but with 3 pharmacists covering 24/7, we simply don’t have capacity." That’s real.Smaller facilities report 37% higher implementation barriers due to staffing. But solutions exist. Automated tools like the FDA’s Sentinel Initiative now push safety alerts directly into EHRs, cutting manual entry by 80%. Mayo Clinic, an early adopter, saw alert processing time drop from 2 hours to 20 minutes per alert.
Another issue: integrating FDA MedWatch alerts. The FDA releases about 120 drug safety updates a year. If your system can’t auto-import them, you’re missing critical updates. By 2025, CMS will require documentation of high-alert protocols to qualify for reimbursement-so delays aren’t just risky, they’re costly.
How to Start
You don’t need a big budget to begin. Start small:- Identify your top 3 high-alert medications based on ISMP’s 2024-2025 list.
- For each, write down the exact safety alert and required action.
- Train staff or family members on how to document it.
- Use free templates from ISMP or AHRQ (available online).
- Set a monthly review: Did any errors happen? Was the alert triggered? Was it bypassed? Why?
It takes 40 staff hours to build a facility-specific list. But the payoff? A 2022 ECRI Institute analysis found that hospitals saved $1.2 million per year by preventing adverse events-far more than the $285,000 annual cost of maintenance.
What’s Next
The future is automation. By 2027, ECRI predicts 75% of U.S. hospitals will use AI-driven systems that auto-classify alerts based on past errors. Epic’s new AI module, launching in Q2 2025, will prioritize alerts using your facility’s own data. But experts like Dr. David Bates warn: "AI must be validated. Early systems had 18% false-negative rates." That means human oversight still matters.For now, the best tool is still a clear, accurate, documented safety alert. No fancy tech required. Just attention to detail. Because when it comes to medication safety, the smallest detail can be the difference between life and death.
What medications are considered high-alert?
High-alert medications are those with a higher risk of causing serious harm if used incorrectly. According to the Institute for Safe Medication Practices (ISMP), these include insulin, opioids (like morphine and fentanyl), anticoagulants (like warfarin and heparin), neuromuscular blockers (like succinylcholine), and oral methotrexate. The 2024-2025 ISMP list includes 19 categories total, and each hospital must create its own facility-specific list based on local usage patterns.
Do I need to document safety alerts if I’m just taking one high-alert medication?
Yes. Even if you’re only on one high-alert drug, documentation is critical. A single error-like taking insulin without checking your blood sugar or taking methotrexate daily instead of weekly-can be fatal. Documenting the alert ensures you (and your providers) remember the specific risks and required actions. For patients, a simple note on your medication list like "Insulin: Always check glucose before dose. Do not give if under 70" is enough.
Can I rely on my pharmacy’s electronic alerts instead of documenting myself?
No. Electronic alerts from pharmacies are helpful, but they’re not foolproof. Studies show that up to 49% of electronic alerts are bypassed without reading, especially if they’re frequent or vague. You need your own documented safety plan-written down and reviewed regularly. Your personal list should include the specific risks and actions, not just "Alert: High Risk."
How often should I update my medication safety documentation?
Update your documentation every time your medication changes-whether it’s a new drug, a dose change, or a discontinued medication. For healthcare facilities, safety committees should review documentation monthly. At minimum, review your personal list during every provider visit and after any hospital discharge. Outdated lists are worse than no lists-they give false confidence.
What if my doctor says I don’t need to document anything?
Trust your instincts. Even if your provider doesn’t emphasize it, documenting safety alerts is a proven way to prevent errors. The Joint Commission and FDA require documentation for accredited hospitals, and the American Society of Health-System Pharmacists (ASHP) gives it their highest recommendation (1A evidence). If you’re unsure, ask: "What’s the specific risk with this medication, and what should I do if something goes wrong?" Write down the answer. It’s your safety.
jared baker
March 20, 2026 AT 03:46Just keep it simple: write down the drug, the risk, and what to do. No fancy charts needed. I’ve seen nurses forget insulin checks because the alert was buried in 12 pop-ups. A sticky note on the fridge? Better than nothing. Your life matters more than EHR compliance forms.
Michelle Jackson
March 20, 2026 AT 13:20Let’s be real - most of these ‘safety alerts’ are just hospital bureaucracy dressed up like lifesaving tech. You think a patient in rural Ohio is going to write ‘double-check by two licensed staff’ on their phone? Please. They’re just trying to remember if they took their pill today. The system is broken, not the patients.
Justin Archuletta
March 21, 2026 AT 19:36Yes!! Exactly!! I’ve been doing this for years - written list, bolded insulin, circled methotrexate, no exceptions!! It’s not hard, it’s just consistent!! And it saved my mom’s life last year!!
jerome Reverdy
March 23, 2026 AT 12:14There’s a real tension here between ‘document everything’ and ‘don’t overwhelm.’ I’ve worked in three hospitals, and the ones that nailed it didn’t use 15-step forms - they used one clear phrase per high-alert med, printed on a laminated card. Nurses carried them in their scrubs. No clicks, no pop-ups, just ‘insulin: check glucose, log result.’ Simple. Human. Effective. The tech is cool, but the paper card? Still wins.
Also, shoutout to the pharmacist who said they can’t document every bypassed alert - that’s not laziness, that’s systemic under-resourcing. We need to fix staffing, not blame the workers.
Stephen Habegger
March 25, 2026 AT 07:06This is one of those topics where the solution is obvious but rarely implemented. Keep it minimal. Keep it visible. Keep it updated. That’s it. No need for AI, no need for 100-page manuals. Just a piece of paper and a habit. You don’t need a system - you need a routine.
Aileen Nasywa Shabira
March 26, 2026 AT 04:48Oh wow, so now we’re treating patients like they’re nuclear reactors? ‘WARNING: CAUSES RESPIRATORY ARREST - PATIENT MUST BE VENTILATED.’ Did we forget that people have lives outside hospitals? My grandma doesn’t know what a neuromuscular blocker is. She knows ‘don’t take this with grapefruit.’ That’s all she needs. This is overengineering fear.
Robin Hall
March 28, 2026 AT 02:16Let’s not ignore the elephant in the room: this entire framework is a corporate compliance theater designed to protect hospitals from lawsuits, not patients from harm. The ISMP guidelines? Paid for by pharmaceutical lobbyists. The Joint Commission mandates? Enforced by auditors who’ve never held a syringe. The 95% barcode compliance stat? It’s cherry-picked from urban academic centers. Rural clinics? They’re being set up to fail so the big EHR vendors can sell more ‘integrated safety modules.’ This isn’t safety. It’s profit.
And don’t get me started on the FDA’s ‘auto-import’ nonsense - who validates those alerts? Who audits the auto-pull from MedWatch? If the system auto-adds a false alert, who’s liable? The nurse? The patient? The coder who didn’t update the ontology? We’re building a house of cards made of legal disclaimers.
Real safety isn’t in a pop-up. It’s in a human who remembers. A nurse who talks to the patient. A pharmacist who calls the pharmacy. A family member who asks, ‘Why are we doing this?’ Not a checklist. Not a hard-stop. A conversation.
AI won’t fix this. Accountability will. And accountability requires someone to be responsible - not a system that logs a click and forgets.
Sanjana Rajan
March 28, 2026 AT 15:17Wow, you all are so naive. This isn’t about safety - it’s about liability. Hospitals don’t care if you live or die. They care if you sue them. That’s why they make you document everything. So when you die, they can say ‘we followed protocol.’ You’re not being protected. You’re being covered.
Robin Hall
March 30, 2026 AT 05:17^This. Exactly. And the FDA pushing auto-imports? That’s just shifting blame upstream. If the algorithm misclassifies a drug, the nurse gets fired. The vendor? Still gets paid. The hospital? Still gets reimbursed. The patient? Still dead. We’re not fixing safety. We’re outsourcing guilt.